

Most pharmacists do not proactively mention prescription discount cards because contractual gag clauses, pharmacy benefit manager restrictions, and financial conflicts of interest prevent or discourage them from doing so. If you ask directly, most pharmacists can tell you the cash price and confirm whether a discount card applies. The responsibility to ask sits with the patient, not the pharmacist.
You might assume that your pharmacist would always tell you when a cheaper option exists for your prescription. In most cases, that does not happen, and it is not necessarily because your pharmacist does not care. A combination of contractual restrictions, financial structures, and operational pressures within the pharmacy system creates a situation where discount card information often does not reach the patient unless the patient asks for it first. Understanding why this happens gives you the context to take a more active role in your own prescription savings.
Gag Order Clauses: Why Pharmacists Often Cannot Speak Up
The most direct reason pharmacists do not mention discount cards is a contractual restriction commonly called a gag clause. These clauses appear in contracts between pharmacies, pharmacy benefit managers (PBMs), and health plans. They explicitly prohibit pharmacists from volunteering information about cheaper cash prices or discount card options when a patient is using insurance to fill a prescription.
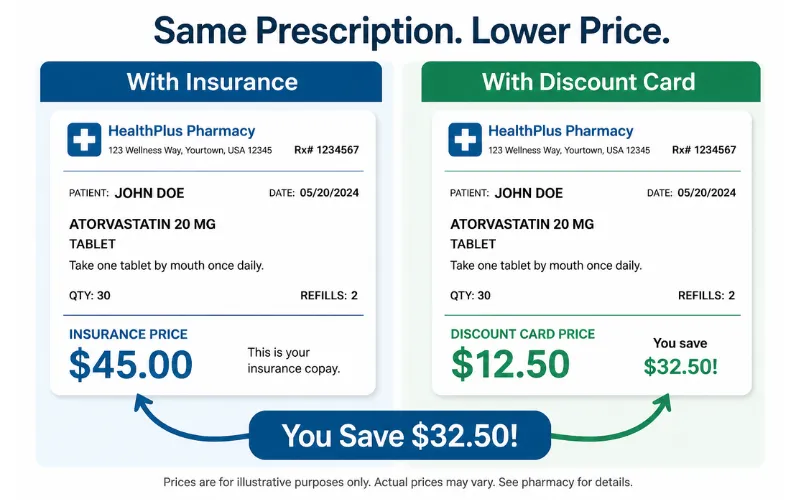
The practical consequence is significant. If your insurance copay for a medication is $45 but the cash price with a discount card is $11, your pharmacist may know this but is contractually barred from telling you unless you ask. Violating a gag clause can result in serious professional consequences for the pharmacist, including removal from the PBM’s pharmacy network, which can represent a substantial portion of a pharmacy’s revenue.
Federal legislation has taken steps toward addressing this. The Know the Lowest Price Act, passed in 2018 for Medicare Part D plans, prohibits gag clauses in contracts involving Medicare-covered drugs and requires pharmacies to tell patients when a lower cost option is available for covered medications.
However, this does not cover all medications or all insurance types, and it does not require pharmacists to proactively discuss discount cards in every transaction. For uninsured patients or those paying out of pocket, knowing which tools reduce prescription costs remains largely the patient’s responsibility to research independently.
How Pharmacy Benefit Managers Shape What You Hear
Pharmacy benefit managers, commonly called PBMs, are the intermediaries that sit between insurance companies, drug manufacturers, and pharmacies. They negotiate drug prices, set formularies, and determine what pharmacies are paid when they dispense a covered medication. Their role in the system is largely invisible to patients but has a direct impact on what information reaches the pharmacy counter.
Several PBM practices create financial conflicts that work against patient transparency. Spread pricing allows a PBM to charge an insurance plan more for a drug than it actually pays the pharmacy, keeping the difference as profit. Copay clawbacks occur when a patient’s copay exceeds the actual cost of the drug, and the PBM retains the overpayment rather than returning it to the patient or pharmacy. Direct and Indirect Remuneration (DIR) fees are charges assessed to pharmacies after a transaction is completed, reducing pharmacy margins in ways that are unpredictable at the time of dispensing.
These financial dynamics create an environment where pharmacies, particularly independent ones, are often more focused on maintaining their relationships with PBM networks than on directing patients toward cash-price options that would route the transaction outside those networks.
When a patient uses a discount card instead of insurance, the transaction bypasses the PBM entirely, which reduces PBM revenue but may benefit the patient significantly. The structural reasons why prescription drug prices stay high in the United States are deeply tied to how PBMs operate within the supply chain.
The Financial Pressure on Independent Pharmacies
Independent pharmacies occupy a particularly difficult position in this system. They operate on thin margins, face declining reimbursement rates from Medicare, Medicaid, and private insurers, and are frequently excluded from lucrative PBM-preferred pharmacy networks. Over 600 independent pharmacies closed in the first nine months of 2025 alone, with closures disproportionately concentrated in Black, Latino, and lower-income communities that already have limited healthcare access.
For an independent pharmacy operating on narrow margins, directing a patient toward a discount card means accepting a lower reimbursement on that transaction and potentially disrupting the insurance billing relationship that covers a portion of the pharmacy’s operating costs. This is not a decision most pharmacists make callously. It is a reflection of the economic reality they operate within. The systemic pressure discourages transparency even when individual pharmacists would prefer to help patients find the lowest price available.
The Reality of Discount Card Pricing
Discount cards deliver genuine savings in many situations, but it is also worth understanding their limitations clearly so you can use them as part of a complete strategy rather than as a universal solution.
For generic medications, discount cards consistently produce prices that are 60 to 80 percent below the standard retail cash price. For brand-name medications, the reduction is meaningful but smaller. How discount cards actually reduce the price at the pharmacy counter is through a pre-negotiated rate network, and those rates vary by pharmacy location, which is why comparing the discount card price at two or three pharmacies before filling always produces better results than using the card at whichever pharmacy is most convenient.
There are also coverage-related limitations to understand. When you use a discount card instead of insurance, the amount you pay does not count toward your insurance deductible or out-of-pocket maximum. For a patient with a $1,000 annual deductible who takes a $200-per-month medication, using a discount card that brings the price to $40 saves money on each individual fill but delays reaching the deductible threshold that would then apply insurance coverage.
Whether the discount card produces a net benefit depends on your specific deductible, the drug’s cost, and how many months remain in the benefit year. Identifying the lowest-cost option for any given prescription requires evaluating both the discount card price and the insurance price in the context of your current deductible status.
The NuLifeSpan Rx Discount Card: Ask for It, Use It, Save Immediately
Since pharmacists often cannot bring up discount cards first, being prepared with one before you arrive at the counter puts the savings in your hands. The NuLifeSpan Rx prescription discount card is completely free, never expires, requires no sign-up, and is accepted at over 35,000 pharmacies nationwide. It delivers savings of up to 80 percent on thousands of covered medications for both human and veterinary prescriptions.
Present it at the counter when you drop off your next prescription and ask the pharmacist to run the price both ways. The discounted price is applied immediately with no paperwork and no claims process.
Privacy Considerations When Using Discount Cards
One aspect of discount card use that receives relatively little attention is data privacy. Prescription discount card programs are not classified as health insurers under most regulatory frameworks, which means they are not always subject to the same HIPAA-level protections that govern insurance companies and pharmacies in their primary insurance-billing capacity.
When you use a discount card, the transaction data, which includes your prescription history, demographics, and purchase patterns, may be collected by the card program operator and used for purposes that go beyond processing the discount. Some programs have historically shared this data with third-party advertisers or data brokers. Privacy policies in this space are frequently written in broad language that permits data use in ways that are not immediately obvious to the average consumer at the point of enrollment or card use.
This does not mean discount cards should be avoided. For most patients, the financial benefit of using a discount card significantly outweighs the data privacy concern, particularly for patients who are already sharing similar data through insurance claims, pharmacy loyalty programs, and other routine healthcare transactions. The practical step is to read the privacy policy of any card program you use before providing personal information during enrollment, and to prefer card programs that clearly state they do not sell health data to third parties.
What to Ask Your Pharmacist Directly
Because pharmacists generally cannot bring up cheaper options proactively, the most effective patient behavior is to ask specific questions directly rather than waiting for the information to be volunteered. The following questions are straightforward, do not require any special knowledge, and will produce useful answers at any pharmacy counter.
- “What is the cash price for this medication without using my insurance?”
- “If I use a prescription discount card, what would the price be?”
- “Is there a generic available for this prescription?”
- “Would a 90-day supply be less expensive per dose than a 30-day supply?”
- “Is this the lowest-cost option available at this pharmacy for this medication?”
Most pharmacists will answer these questions directly and helpfully when asked. The constraint is on volunteering the information, not on answering when a patient initiates the conversation. Making these questions a routine part of every prescription pickup gives you access to information that would otherwise remain invisible behind the counter.
Knowing which specific questions to ask at a major retail pharmacy makes each interaction more productive and ensures you are not leaving savings on the table through an assumption that the price you were quoted is the best available.
The Broader System That Keeps Patients in the Dark
The gag clause issue is one visible symptom of a larger structural problem. Prescription drug pricing in the United States involves multiple layers of intermediaries, each with its own financial incentives, and very few of those incentives are aligned with helping the patient find the lowest possible price. PBMs profit from the spread between what they charge plans and what they pay pharmacies. Manufacturers maintain high list prices to create room for rebates that never reach patients. Retail pharmacies generate margin from proprietary or preferred products rather than the most affordable generics.
Discount card programs exist as a workaround to this system. They bypass the PBM layer and access negotiated rates directly, which is why they can produce prices that are dramatically lower than what the insurance billing process delivers. Why the same drug costs different amounts at different pharmacy locations is a direct result of this fractured and non-standardized pricing structure.
Understanding the system does not require becoming a healthcare policy expert. It requires knowing that the price you are automatically quoted is almost never the lowest available price, and that a single direct question at the counter, combined with a free discount card in your wallet, is usually enough to access a significantly better one. The same dynamic applies to pet prescriptions, where veterinary clinic pricing is even less regulated and the savings from filling at a retail pharmacy with a discount card are often larger than the savings available on human prescriptions.
NuLifeSpan Rx Pet Prescriptions: Savings Your Vet Probably Did Not Mention
Veterinary clinics face the same financial pressures and PBM-adjacent dynamics that keep savings information from reaching patients at human pharmacies, often to an even greater degree. The NuLifeSpan Rx pet prescriptions savings program gives pet owners access to the same free discount card that works for human prescriptions, accepted at participating retail pharmacies for veterinary medications including insulin, thyroid drugs, allergy treatments, and pain management medications.

Ask your veterinarian for a written prescription at your next appointment. Fill it at a retail pharmacy with the NuLifeSpan Rx card. Pay a fraction of what the clinic would have charged for the same drug.
Frequently Asked Questions
Why do pharmacists not tell you about cheaper prescription options?
The primary reason is contractual. Gag clauses embedded in agreements between pharmacies and pharmacy benefit managers prohibit pharmacists from proactively disclosing cheaper cash prices or discount card options when a patient is filling a prescription through insurance. Pharmacists who violate these clauses risk removal from the PBM’s pharmacy network, which is a significant financial consequence. Federal legislation has addressed this partially for Medicare-covered drugs, but the protection does not extend to all medications or all patient populations. The practical takeaway is that asking directly is the most reliable way to surface lower-cost options that would otherwise go unmentioned.
What is a pharmacy gag clause?
A pharmacy gag clause is a contractual provision that prevents a pharmacist from telling a patient that a cheaper option exists for their prescription. These clauses typically appear in contracts between pharmacies and pharmacy benefit managers and have historically been used to prevent pharmacists from mentioning that the cash price for a medication is lower than the patient’s insurance copay. The Know the Lowest Price Act of 2018 prohibited gag clauses in Medicare Part D pharmacy contracts, but similar protections do not apply universally across all insurance types and medications.
Can I ask my pharmacist about discount card pricing even if they did not bring it up?
Yes, and you should. Pharmacists can answer direct questions about cash pricing and discount card options even when they cannot raise the topic proactively. The restriction is on volunteering the information, not on responding honestly when asked. The most effective questions to ask are: what is the cash price without insurance, what would the price be with a discount card, and whether a generic is available. These questions take less than a minute to ask and frequently result in a meaningfully lower price than the one originally quoted.
Do discount cards really save money or are the savings inflated?
Discount cards produce genuine savings in most cases, particularly for generic medications where reductions of 60 to 80 percent below the retail cash price are common and verifiable. The savings figures advertised by discount card programs are sometimes calculated by comparing the discounted price to an inflated reference retail price, which can make the percentage discount look larger than it feels in absolute dollar terms. The most reliable way to evaluate a discount card’s value is to compare the specific price it produces for your specific medication at your local pharmacy against both the retail cash price and your insurance copay, rather than relying on advertised percentage savings figures.
Does using a discount card affect my insurance deductible?
Yes. When you pay for a prescription using a discount card instead of your insurance, the amount you pay does not count toward your insurance deductible or annual out-of-pocket maximum. This is a meaningful consideration for patients on high-deductible plans who are actively working toward meeting their deductible. If you are close to meeting your deductible, using insurance even at a higher per-fill cost may make more financial sense in the long run because it counts toward the threshold that activates insurance coverage. If you are early in the benefit year and far from your deductible, the discount card price is often lower than the pre-deductible insurance price for the same medication.
Are there privacy risks to using a prescription discount card?
There are privacy considerations worth understanding. Prescription discount card programs are not always subject to the same HIPAA protections that govern insurance companies and pharmacies in their primary insurance-billing role. Some programs collect prescription history, demographic data, and purchase patterns and may share or sell this data to third-party advertisers or data analytics companies. The privacy policy of any card program you use is worth reviewing before providing personal information during enrollment. Programs that explicitly state they do not sell health data to third parties offer a meaningfully stronger privacy commitment than those using broad or vague data-use language.
What is a pharmacy benefit manager and how do they affect my drug costs?
A pharmacy benefit manager (PBM) is a company that acts as an intermediary between insurance plans, drug manufacturers, and pharmacies. PBMs negotiate drug prices, design the formularies that determine which drugs are covered by a plan, and set the rates that pharmacies are paid when they dispense a covered medication. Several PBM practices increase costs for patients and pharmacies without direct transparency. Spread pricing allows PBMs to charge insurance plans more for a drug than they pay the dispensing pharmacy, keeping the difference as profit. Copay clawbacks occur when a patient’s copay exceeds the drug’s actual cost, with the excess retained by the PBM rather than refunded to the patient or pharmacy. These practices are a significant driver of the gap between a drug’s actual cost and what patients pay at the counter.
How can I make sure I am always getting the lowest prescription price?
The most reliable routine combines three habits: always carrying a free prescription discount card, always asking the pharmacist to check both the insurance price and the cash price with the card before completing the transaction, and comparing prices at two or three pharmacies before filling any new or high-cost prescription rather than defaulting to the most convenient location. This same approach applies to pet prescriptions, where filling at a retail pharmacy with a discount card instead of at the veterinary clinic typically produces the lowest available price on any medication your vet can prescribe in writing. Consistent application of these three habits on every fill produces cumulative savings that compound significantly over the course of a year.
Conclusion
Your pharmacist’s silence about discount cards is rarely a reflection of indifference. It is almost always the product of contractual restrictions, PBM financial relationships, and operational pressures that make proactive disclosure difficult or economically risky. The system is not designed to surface the lowest price for you automatically. It is designed to process transactions efficiently within a set of financial arrangements that do not prioritize patient savings.
The solution is simple and requires no expertise: ask directly, carry a free discount card, and compare prices before you commit to any fill. These three actions put the information that pharmacists cannot volunteer into your hands before you reach the counter. Visit the NuLifeSpan Rx blog for more guides on specific medications, pharmacy strategies, and savings tools designed for every patient and every budget.









{kind=link}